HIV Pre-Exposure Prophylaxis (PrEP) Online Course at Coursera Review. Day 8 of 42.
 Online Course at Coursera Review. Day 8 of 42. - صورة 1")
Let continue our journey into HIV prophylaxis with the PrEParing online course introduced by Coursera MOOC platform and Johns Hopkins University. Today is day 8 of 42, and we will be reviewing the lecture “PrEP and nPEP for HIV Prevention: Case Studies.” This lecture was delivered by Dr. Joyce Leitch Jones, Associate Professor of the Department of Infectious Diseases at the Johns Hopkins University School of Medicine (USA).
Dr. Jones begins her talk disclosing the conflicts of interests saying she has no conflict of interest, no personal contracts with pharmaceutical companies or other organizations, and the lecture is an independent review of best practices in HIV prevention.
Disclosing the conflict of interests is an integral part of a scientific speech or article, particularly in medicine because it is important for people to accept an honest and up-to-date review of the topic. The presence of contracts with individual stakeholders may distort the real picture. Dr. Jones disclosed there is no conflict of interests so we tend to believe her.
Joyce begins the lecture with a story about the differences between HIV pre-exposure prophylaxis, PrEP, and nonoccupational post-exposure prophylaxis, nPEP.
PrEP
PrEP involves a daily intake of an antiretroviral drug before HIV infection for someone without HIV who are at high risk of getting HIV from another person. To prescribe a PrEP course, the doctor makes sure a patient is HIV negative and only then prescribes one pill once a day to prevent possible transmission of HIV in a case of dangerous contact with an HIV-positive individual. The course continues until the risk of HIV transmission is high and as long as patient remain HIV negative.
nPEP
Nonoccupational post-exposure prophylaxis, nPEP, involves taking a combination of antiretroviral medication within 72 hours after exposure to HIV, best as soon as possible. Patients have to take two to three pills a day for 28 days after the exposure and then stop after 28 days. At that point, if the person remains at high risk for HIV infection then the doctor would consider switching the patient to PrEP.
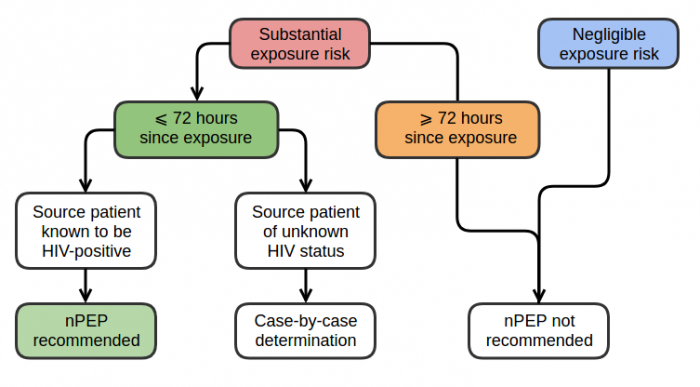
Figure 1 — Algorithm or evaluating patients who have had a possible nonoccupational exposure to HIV.
In the next slide, the lecturer shows a slide (Figure 1), which illustrates an algorithm for choosing tactics in case a person immediately came to a doctor after a dangerous contact with an HIV-positive individual. Such an algorithm contrasts prescribing PEP in the case of occupational exposure to HIV among healthcare workers and other persons who work with bodily fluids and are potentially exposed to HIV through their work.
In the situation of non-occupational risk, the doctor first determines whether the risk of HIV transmission is substantial or negligible.
For those patients who are at substantial risk for HIV acquisition, particular risks of substantial exposure to HIV includes exposure of the:
- vagina;
- rectum;
- eye;
- mouth or other mucous membranes;
- non-intact skin or percutaneous contact with blood, semen, vaginal secretions, rectal secretions, breast milk or any bodily fluid that is visibly contaminated with blood when the source person is known to be HIV positive.
The negligible risk for HIV acquisition includes exposure of those same mucous membranes, so vagina, rectum, eye, mouth or other mucous membranes with intact or non-intact skin, or percutaneous contact with bodily secretions that do not pose a risk for HIV transmission. So those bodily secretions include urine, nasal secretions, saliva, sweat or tears if they are not visibly contaminated with blood.
It does not matter — whether or not the source person is HIV or not, statistics show that the average risk is negligible.
You could see from the diagram that in the case of negligible risk nPEP is not recommended. nPEP is prescribed only in case of substantial risk if less than 72 hours have passed since the dangerous contact and it was known that the partner is HIV-positive.
In the case when a dangerous contact occurred less than 72 hours ago, but the partner’s HIV status is not known, the doctor asks the patient additional questions and makes an individual decision — whether to prescribe nPEP or not.
So remember, PrEP is pre, so that means before exposure to HIV, taking Truvada once a day before exposure to HIV versus nPEP which involves taking combination antiretroviral medications within 72 hours after the substantial risk of exposure to HIV.
In the next few slides, Dr. Jones presented a couple of clinical cases to make us think about the choice — whether the doctor should prescribe PrEP, nPEP or nothing.
In the first case, a 24-year-old man who had sex with three men and two women one day ago. He engaged in vaginal sex, oral and anal sex in both receptive and insertive intercourse and did not use condoms. The man is unsure of the HIV status of any of his sexual partners and claims that the last HIV test was performed one month ago by the modern 4th generation antigen-antibody test system, the result was negative.What would you recommend to this man? PrEP or nPEP?
Let’s take a look at the algorithm. Does the man have a substantial risk of HIV transmission? Definitely, yes, because he had exposure of his rectum and his mouth, and other mucous membranes so in this case the penis with semen and vaginal secretions. It is unknown whether any of his partners was HIV-positive or not. Since the contact was less than 72 hours and we do not know if there was HIV in the patient’s body at the time of sexual intercourse, the algorithm leads to an individual selection of the prevention strategy. This is where you come to case by case determination.
Dr. Joyce Jones recommended thinking about the prevalence of HIV within the community. If this man lives in a place where the prevalence of HIV is high, Joyce would rather prescribe nPEP in this case.
After deciding to prescribe nPEP, Joyce would have made an HIV test for this patient, prescribed blood sampling for liver function analysis and serology for hepatitis B, hepatitis C, syphilis, gonorrhea. If there were a woman, a pregnancy test would be required and if the woman is not pregnant — Plan B would be assigned for pregnancy prevention.
The recommended regimens for nPEP is a combination of two antiretroviral drugs. The first is Truvada — tenofovir disoproxil fumarate and emtricitabine. The second is Raltegravir or Dolutegravir. It will be necessary to make sure the doctor gave a patient adherence counseling. On the other hand, the patient’ responsibility is proper daily pills intake during the 28 days of the nPEP course.
As Joyce has already noted, if the patient remains dangerous behavior after completing the nPEP course, he or she will be recommended switching to PrEP to reduce the risk of HIV transmission in the future.
Dr. Joyce Jones introduced the second clinical case.
Again a 24-year-old man who had sex with three men and two women three months ago. He reports engaging in the same sexual activity as in the first case, and the last HIV test was made one month ago with a negative result.What would you recommend to this man? PrEP or nPEP?
Again, let’s return to the algorithm. As in the first case, the risk is substantial. However, the patient asked for a medical consultation much later. Therefore, in this case, nPEP is not recommended.
But if the HIV test is negative for such a man, the doctor could also prescribe PrEP. To do so, the doctor needs to ask a few questions — does this patient continues or plans unprotected sexual intercourses with several partners? Are there other circumstances in his/her life allowing to be attributed to a high-risk group, such as injecting drug use, commercial sex, or a permanent relationship with an HIV-positive partner? An affirmative answering to one of these questions could potentially benefit for PrEP.
Let’s sum up.
PrEP is recommended to people of all genders if there is a recent history of:
- one-time or regular sex with an HIV-positive partner;
- STI — a sexually transmitted bacterial infection;
- a high number of sexual partners;
- an episode of sexual intercourse, in which the condom was not used or used inconsistently;
- providing commercial sex services;
- injecting drugs and having an HIV-positive partner who also uses drugs;
- injecting drugs and sharing injection equipment;
After the doctor assesses the risks for acquiring HIV and it looks like the patient could benefit from PrEP, a clinical check-up is necessary.
The doctor has to ensure that the patient is HIV negative, have no signs and symptoms of acute HIV infection, check renal function, Hepatitis B status. If the patient is clinically eligible, there’s another testing that should be done and other counseling that should be done that is reviewed in the next lectures of the PrEParing online course.
If no contraindications to PrEP are identified, and the patient gives informed consent, the physician proceeds to provide all of the appropriate supportive services and counseling and risk reduction counseling the next phase of the consultation.
That's a summary for how PrEP is prescribed.
Today the story turned out to be long, and we hope that you read it with unconcealed curiosity and have questions. The instructors of the PrEParing online course and we at the Life4me+ mobile app for HIV-positive persons want you to have a clear understanding of the difference between PrEP and nPEP as methods of preventing HIV infection.
Tomorrow you will be the ninth day of the course, a second day of the second module, in which we will immerse ourselves deeper into the PrEP discussing the pharmacokinetics and pharmacodynamics of the Truvada in the human body.
If you have not already signed up for the PrEParing course on the Coursera platform — it’s never too late. Just go to https://www.coursera.org/learn/prep.
Stay with us and stay healthy!



